-
About
-
Neuro-Lab
-
RTalk
-
Rehab-Institube
-
Community
Digital-Learning
본문
해당 강좌는 수강종료 상태 입니다.
수강신청 후 관련 강의영상을 시청 하실 수 있습니다.Gait
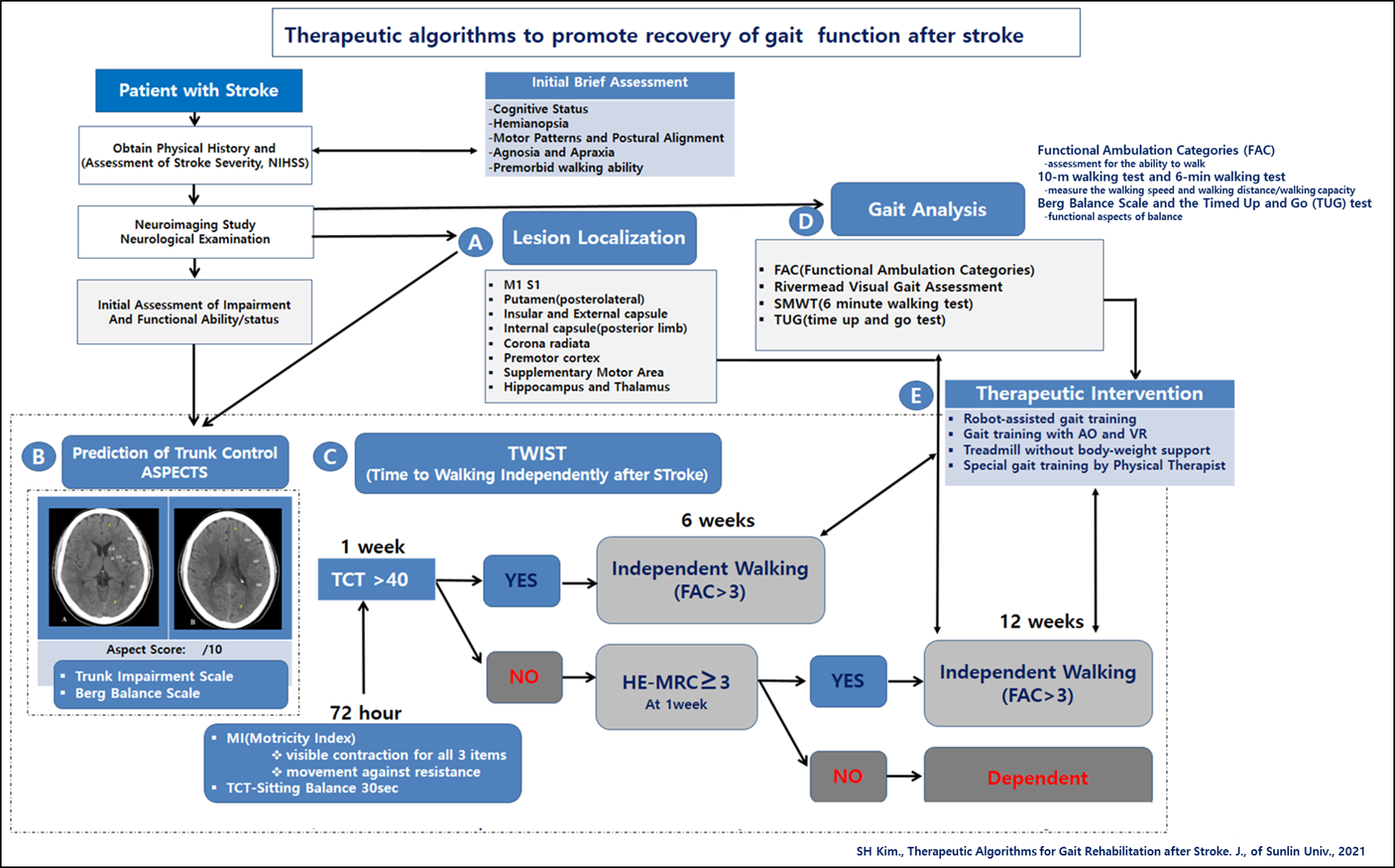
Predicting functional recovery after a stroke is very important. Predicting the degree of functional recovery can establish a patient\'s treatment prognosis and provide a clinical scientific basis for the clear application of patient-centered, targeted therapies. The degree of motor function impairment and the potential for motor function recovery is closely related to the lesion site, size, and degree of the lesion. Therefore, clinical therapists should be able to plan a rehabilitation strategy suitable for each patient through neuroimaging analysis that can identify the patient\'s brain injury area and establish and apply a clear symptom-based therapeutic intervention strategy.
The brain regions associated with human gait have been found to be important in the complementary motor area, the pre-complementary motor area, the premotor cortex, and the pre-frontal area (Suzuki et al., 2008; Harada et al., 2009).
An area that plays an important role in the recovery of walking function after stroke is the premotor cortex area. According to a study by Miyai et al. (2002), it was confirmed that the activity of the premotor cortex and the pre-complementary motor area of the damaged brain hemisphere was increased with ambulatory treatment after stroke. Later studies have confirmed that the active area of the brain during walking in the early stages of injury becomes active in the premotor cortex and complementary motor area of the undamaged brain hemisphere, but after rehabilitation, it becomes more active in the premotor cortex and complementary motor area of the injured brain hemisphere (Miyai et al., 2003).
The corticospinal tract originates mainly from the primary motor cortex, and damage to the corticospinal tract has been reported to be closely related to functional impairment of the upper limbs, including general damage to the body (Puig et al., 2010; Feng et al., 2015). The corticospinal tract has very different functions depending on the brain region originating: 1) the corticospinal cord originating in the primary motor cortex is responsible for motor execution, 2) the cortical spinal cord originating from the complementary motor region is internally generating movement planning and coordination, 3) the cortical spinal cord originating in the premotor cortex is involved in the planning and coordination of visually-guided movements, and 4) the cortical spinal cord originating in the somatosensory cortex is involved in the downward regulation of afferent inputs generated by movement (Jang,
2014). Damage to the corticospinal cord on the hemisphere side of the brain has been found to cause more severe gait deficits in severe cases (Jayaram et al., 2012). The results also confirmed that there were more behavioral deficits in patients with large ipsilateral connectivity. Neuroanatomically and physiologically, the corticospinal tract originates in the premotor and complementary motor areas, but it also forms a cortico-reticular pathway to regulate the functions of the trunk and proximal upper limbs through the regulation of the reticular formation cortical-reculospinal tracts in the cortical. In addition, when it comes to hand function, these areas also play an important role in reaching and grasping.
There is an interesting brain schematic study related to gait recovery after stroke. According to a study by Kim et al. (2018), 1) the posterior limb of the internal capsule is closely related to the increase in walking speed and the extension of the knee canal in the standing phase, 2) the hippocampus and frontal lobe are closely related to the number of steps per minute (cadence), 3) the proximal corona radiata is closely related to the stride length and the maximum extension angle of the injured hip joint at the time of standing, 4) the paracentral lobule is closely related to the maximum flexion angle of the knee joint involved in the swing phase and the maximum angle of instep bending of the ankle invaded in the standing phase,
5) The frontal lobe, thalamus, and lentiform nucleus have been found to be closely related to the kinetic parameter. Hippocampal lesions are closely related to a decrease in the number of walks and function as a very important area for reproducing movement patterns during walking (Beauchet et al., 2018; Kindred et al., 2015). Postolateral putamen is closely related to asymmetric gait (Alexander et al., 2009), and cerebral and basal ganglia are found to be closely related to motor deficits of the lower extremities (Moon et al., 2016). With regard to changes in gait symmetry, putamen, insular, and external capsules are closely related to asymmetric gait (Alexander et al., 2009), and basal ganglia, brain islets, secondary somatosensory areas or complementary motor areas, and premotor cortex have been found to be associated with lower limb motor defects (Mihara et al., 2012).
#Gait #MRI #Algorithm #Stroke
부가 정보
김식현
2023/10/21 13:08 ~
12/30 18:53
신청(결제)일로 부터 7일
100,000원
로그인 후 신청 및 확인이 가능 합니다.
- 교육시작 전(당일전날) 전액(100%) 환불
- 교육시작 후(당일포함) 환불 없음